Gemigliptin tartrate sesquihydrate, metformin hydrochloride.
Each tablet contains: Active ingredient: Gemigliptin tartrate sesquihydrate 68.9 mg (in-house, equivalent to gemigliptin pure free base 50 mg), Metformin hydrochloride (EP) 1 g.
Excipients/Inactive Ingredients: Microcrystalline Cellulose, Magnesium Stearate, Opadry II 85F34790, Croscarmellose Sodium, Polyvinyl Acetate Aqueous Dispersion 30%, Stearyl Fumarate Sodium, Hypromellose.
Gemigliptin/Metformin HCl is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
As initial therapy for treatment naïve patients with inadequate glycemic control by diet and exercise alone.
In patients with inadequate glycemic control with the maximal tolerated dose of metformin alone.
In combination with sulfonylurea in patients inadequately controlled on their maximal tolerated dose of metformin and a sulfonylurea.
In combination with insulin in patients with inadequate glycemic control with insulin monotherapy or insulin/metformin dual therapy.
In patients already receiving an identical combination of gemigliptin and metformin as separate tablets.
Dosage of Gemigliptin/Metformin HCl must be individualized on the basis of the patient's current regimen, effectiveness, and tolerability. Gemigliptin/Metformin HCl should generally be administered once daily with a meal in the evening and the dosage should be gradually escalated to reduce the gastrointestinal side effects associated with the metformin component.
Patients taking Gemigliptin/Metformin HCl 50 mg/500 mg or 50 mg/1 g should take one tablet once daily.
Patients taking Gemigliptin/Metformin HCl 25 mg/500 mg or 25 mg/1 g should take two tablets once daily.
The recommended starting dose of Gemigliptin/Metformin HCl in patients who need 50 mg of gemigliptin and who are not currently treated with metformin is 50 mg gemigliptin and 500 mg metformin extended-release once daily with gradual dose escalation to reduce the gastrointestinal side effects due to metformin.
For patients with inadequate glycemic control on metformin monotherapy or for patients with inadequate glycemic control on dual combination of metformin and sulfonylurea or metformin and insulin, the recommended daily dose of Gemigliptin/Metformin HCl is 50 mg gemigliptin and the dose of metformin already being taken. When switching from metformin immediate-release to metformin extended-release, glycemic control should be closely monitored and the dose adjusted on the basis of blood glucose measurements.
When used in combination with a sulfonylurea or insulin, a lower dose of the sulfonylurea or insulin may be required to reduce the risk of hypoglycemia.
For patients switching from co-administration of gemigliptin and metformin, Gemigliptin/Metformin HCl should be initiated at the dose of gemigliptin and metformin already being taken. When switching from metformin immediate release to extended release, glycemic control should be closely monitored and the dose adjusted on the basis of blood glucose measurements.
The maximum recommended daily dose is 50 mg gemigliptin and 2000 mg metformin extended-release.
No studies have been performed specifically examining the safety and efficacy of Gemigliptin/Metformin HCl in patients previously treated with other oral anti-hyperglycemic agents and switched to Gemigliptin/Metformin HCl. Any change in therapy of type 2 diabetes should be undertaken with care and appropriate monitoring as changes in glycemic control can occur.
Gemigliptin/Metformin HCl should be swallowed as a whole and it must not be split, crushed, or chewed before swallowing.
Gemigliptin: During clinical trials in healthy subjects, multiple doses of up to 600 mg gemigliptin were administered for duration of 10 days. One case of increased heartbeat was observed at a single dose of 600 mg gemigliptin. There is no experience with daily doses above 600 mg in clinical studies. In the event of an overdose, it is reasonable to employ the usual supportive measures, e.g., remove unabsorbed material from the gastrointestinal tract, employ clinical monitoring (including obtaining an electrocardiogram), and institute supportive therapy as indicated by the patients clinical status.
Metformin: Overdose of metformin hydrochloride has occurred, including ingestion of amounts greater than 50 grams. Hypoglycemia was reported in approximately 10% of cases, but no casual association with metformin hydrochloride has been established. Lactic acidosis has been reported in approximately 32% of metformin overdose cases. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
Metformin: Can rarely cause severe lactic acidosis.
Can rarely cause hypoglycemia in patients taking insulin, sulfonylurea, and other antidiabetic medications.
Precautions for use: Patients with a history of serious hypersensitivity reactions, i.e., angioedema or anaphylaxis, to the active substances or to any of the excipients of this medication or another dipeptidyl peptidase-4 (DPP4) inhibitor.
Renal impairment (e.g., serum creatinine levels ≥15 mg/dL for men, ≥14 mg/L for women or abnormal creatinine clearance), which may also result from conditions such as cardiovascular collapse (shock), acute myocardial infarction, and septicemia.
Patients with congestive heart failure requiring medication.
Radiologic studies including the use of intravascular iodinated contrast materials (for example, intravenous urogram, intravenous cholangiography, angiography, and computed tomography) can lead to acute alteration of renal function and have been associated with lactic acidosis in patients receiving products containing metformin. Therefore, in patients in whom any such study is planned, this drug should be discontinued at least 48 hours prior to the procedure, and withheld for 48 hours subsequent to the procedure and reinstituted only after renal function has been re-evaluated and found to be normal.
Patients with type 1 diabetes or acute or chronic metabolic acidosis, including diabetic ketoacidosis, with or without coma, or history of ketoacidosis (Type 1 diabetes and diabetic ketoacidosis should be treated with insulin).
Pre-diabetic coma.
Known hypersensitivity to components of this drug or biguanides.
Therapy should be temporarily suspended in patients with severe infection or traumatism and should not be restarted until the patient's oral intake has resumed and renal function has been evaluated as normal.
Therapy should be temporarily discontinued 48 hours prior to any surgical procedure (except minor procedures not associated with restricted intake of food and fluids), and withheld for at least 48 hours subsequent to the procedure and reinstituted only after renal function has been re-evaluated and found to be normal.
Debilitated, malnourished or starved patients, and those with adrenal or pituitary insufficiency.
Patients with hepatic impairment (because patients with hepatic impairment has been associated with some cases of lactic acidosis, use of this drug should be avoided in patients with clinical or laboratory evidence of hepatic impairment), pulmonary infarction, severe respiratory insufficiency, and any conditions that induce hypoxemia, excessive alcohol, dehydration, gastrointestinal symptoms such as diarrhea and vomiting.
Pregnant or potentially pregnant women and nursing mothers.
Caution should be exercised when Gemigliptin/Metformin HCl is administered to: Metformin (Possibility of lactic acidosis and hypoglycemia): Irregular diet, lack of food intake; Intense muscle exercise; Patients taking drugs that interact with metformin.
Acute pancreatitis: Pancreatitis has been reported in the patients treated with gemigliptin. Therefore, patients should be informed of the characteristic symptoms of acute pancreatitis such as persistent, severe abdominal pain. If pancreatitis is suspected, administration of gemigliptin should be discontinued and this product should not be restarted. Caution should be exercised in patients with a history of pancreatitis.
General Precautions: Lactic Acidosis: Lactic acidosis is a serious, metabolic complication that can occur due to metformin accumulation during treatment with Gemigliptin/Metformin HCl and is fatal in approximately 50% of cases. Lactic acidosis may also occur in association with a number of pathophysiologic conditions, including diabetes mellitus, and whenever there is significant tissue hypoperfusion and hypoxemia. Lactic acidosis is characterized by elevated blood lactate concentrations (>5 mmol/L), decreased blood pH, electrolyte disturbances with an increased anion gap, and an increased lactate/pyruvate ratio. When metformin is implicated as the cause of lactic acidosis, metformin plasma levels >5 ug/mL are generally found.
The reported incidence of lactic acidosis in patients receiving metformin hydrochloride is fairly low (approximately 0.03 cases/1000 patient-years, with approximately 0.015 fatal cases/1000 patient-years). In more than 20,000 patient-years exposure to metformin in clinical trials, there were no reports of lactic acidosis. Reported cases have occurred primarily in diabetic patients with significant renal impairment, including both intrinsic renal disease and renal hypoperfusion, often in the setting of multiple concomitant medical/surgical problems and multiple concomitant medications. Patients with congestive heart failure requiring pharmacologic management, in particular those with unstable or acute congestive heart failure who are at risk of hypoperfusion and hypoxemia, are at increased risk of lactic acidosis. The risk of lactic acidosis increases with the degree of renal dysfunction and the patient's age. The risk of lactic acidosis may, therefore, be significantly decreased by regular monitoring of renal function in patients taking metformin. In particular, treatment of the elderly should be accompanied by careful monitoring of renal function. Metformin treatment should not be initiated in patients ≥80 years of age unless measurement of creatinine clearance demonstrates that renal function is not reduced. In addition, metformin should be promptly withheld in the presence of any condition associated with hypoxemia, dehydration, or sepsis. Because impaired hepatic function may significantly limit the ability to clear lactate, metformin should generally be avoided in patients with clinical or laboratory evidence of hepatic impairment. Patients should be cautioned against excessive alcohol intake when taking metformin, because alcohol potentiates the effects of metformin on lactate metabolism. In addition, metformin should be temporarily discontinued prior to any intravascular radiocontrast study and for any surgical procedure.
The onset of lactic acidosis often is subtle, and accompanied only by nonspecific symptoms such as malaise, myalgias, respiratory distress, increasing somnolence, and nonspecific abdominal distress. There may be associated hypothermia, hypotension, and resistant bradyarrhythmias with more marked acidosis. Patients should be educated to promptly report these symptoms to their physician should they occur. If present, metformin should be withdrawn until lactic acidosis is ruled out. Serum electrolytes, ketones, blood glucose, blood pH, lactate levels, and blood metformin levels may be useful. Once a patient is stabilized on any dose level of metformin, gastrointestinal symptoms, which are common during initiation of therapy, are unlikely to recur. Later occurrence of gastrointestinal symptoms could be due to lactic acidosis or other serious disease.
Levels of fasting venous plasma lactate above the upper limit of normal but less than 5 mmol/L in patients taking metformin do not necessarily indicate impending lactic acidosis and may be explainable by other mechanisms, such as poorly-controlled diabetes or obesity, vigorous physical activity, or technical problems in sample handling.
Lactic acidosis should be suspected in any diabetic patient with metabolic acidosis lacking evidence of ketoacidosis (ketonuria and ketonemia).
Lactic acidosis is a medical emergency that must be treated in a hospital setting. In a patient with lactic acidosis who is taking metformin, the drug should be discontinued immediately and general supportive measure promptly instituted. Because metformin hydrochloride is dialyzable (with a clearance of up to 170 mL/min under good hemodynamic conditions), prompt hemodialysis is recommended to correct the acidosis and remove the accumulated metformin. Such management often results in prompt reversal of symptoms and recovery.
Monitoring of renal functions: Metformin is known to be substantially excreted by the kidney and the risk of metformin accumulation and lactic acidosis increases with the degree of impairment of renal function. Thus, patients with serum creatinine levels above the upper limit of normal for their age should not receive Gemigliptin/Metformin HCl.
Before initiation of Gemigliptin/Metformin HCl and at least annually thereafter, renal function should be assessed and verified as normal. In patients in whom development of renal dysfunction is anticipated (for example, patients with advance age), renal function should be assessed more frequently and Gemigliptin/Metformin HCl discontinued if evidence of renal impairment is present.
Impaired hepatic function: Impaired hepatic function has been associated with some cases of lactic acidosis. Gemigliptin/Metformin HCl should generally be avoided in patients with clinical or laboratory evidence of hepatic disease.
Vitamin B12 levels: In controlled clinical trials of metformin of 29 weeks duration, a decrease to subnormal levels of previously normal serum vitamin B12 levels, without clinical manifestations, was observed in approximately 7% of patients. Such decrease, possibly due to interference with B12 absorption from B12-intrinsic factor complex, is, however very rarely associated with anemia and appears to be rapidly reversible with discontinuation of metformin or vitamin B12 supplementation. Measurement of hematologic parameters on an annual basis is advised in patients on Gemigliptin/Metformin HCl and any apparent abnormalities should be appropriately investigated and managed.
Certain individuals (those with inadequate Vitamin B12 or calcium intake or absorption) appear to be predisposed to developing subnormal Vitamin B12 levels. In these patients, routine serum Vitamin B12 measurements at two-to three-year intervals may be useful.
Alcohol intake: Alcohol is known to potentiate the effect of metformin on lactate metabolism. Therefore, should not consume alcohol while receiving Gemigliptin/Metformin HCl.
Surgical procedures: Therapy should be temporarily discontinued at the time of or prior to any surgical procedure (except minor procedures not associated with restricted intake of food and fluids), and should not be restarted until the patients oral intake has resumed and renal function has been evaluated as normal.
Change in clinical status of patients with previously controlled type 2 diabetes: A patient with type 2 diabetes previously well controlled on Gemigliptin/Metformin HCl who develops laboratory abnormalities or clinical illness (especially vague and poorly defined illness) should be evaluated promptly for evidence of ketoacidosis or lactic acidosis. Evaluation should include serum electrolytes and ketones, blood glucose and, if indicated, blood pH, lactate, pyruvate, and metformin levels. If acidosis of either form occurs, metformin must be stopped immediately and other appropriate corrective measure initiated.
Hypoglycemia: Gemigliptin: Hypoglycemia has been observed when gemigliptin was used in combination with a sulfonylurea. Therefore, to reduce the risk of hypoglycemia caused by sulfonylurea, a lower dose of sulfonylurea may be considered.
Metformin: Hypoglycemia does not occur in patients receiving metformin alone under usual circumstances of use, but could occur when caloric intake is deficient, when strenuous exercise is not compensated by caloric supplementation, or during concomitant use with other glucose-lowering agents (such as sulfonylureas and insulin) or ethanol. Elderly, debilitated, or malnourished patients and those with adrenal or pituitary insufficiency or alcohol intoxication are particularly susceptible to hypoglycemic effects. Hypoglycemia may be difficult to recognize in the elderly, and in people who are taking beta-adrenergic blocking drugs.
Concomitant medications affecting renal function or metformin disposition: Concomitant medication(s) that may affect renal function or result in significant hemodynamic change or may interfere with the disposition of metformin, such as cationic drugs that are eliminated by renal tubular secretion, should be used with caution.
Radiologic studies involving the use of intravascular iodinated contrast materials: Iodinated contrast materials can lead to acute alteration of renal function and have been associated with lactic acidosis in patients receiving this drug. Therefore, in patients in whom any such study is planned, this drug should be temporarily discontinued at the time of or prior to the procedure, and withheld for 48 hours subsequent to the procedure and reinstituted only after renal function has been re-evaluated and found to be normal.
Hypoxic states: Cardiovascular collapse (shock), acute congestive heart failure, acute myocardial infarction and other conditions characterized by hypoxemia have been associated with lactic acidosis and may also cause prerenal azotemia. When such events occur in patients on metformin therapy, Gemigliptin/Metformin HCl should be promptly discontinued.
Severe and disabling arthralgia: There have been post-marketing reports of severe and disabling arthralgia in patients taking other DPP-4 inhibitors. The time to onset of symptoms following initiation of drug therapy varied from one day to years. Patients experienced relief of symptoms upon discontinuation of the medication. A subset of patients experienced a recurrence of symptoms when restarting the same drug or a different DPP-4 inhibitor. Consider DPP-4 inhibitors as a possible cause for severe joint pain and discontinue drug if appropriate.
Bullous pemphigoid: Bullous pemphigoid requiring hospitalization was reported in the post-marketing surveillance in the patients who took other DPP-4 inhibitors. The patients recovered in general after the stop of the DPP-4 inhibitors administration and the use of local or general immunosuppressants. It should be notified to the patients if the patients experience blisters or erosions, it should be notified to their doctors. If bullous pemphigoid is suspected, please stop taking this medical product and consult dermatologists for diagnosis and proper treatment.
Hypersensitivity Reaction: There have been postmarketing reports of severe hypersensitivity reactions in patients treated with gemigliptin including Stevens-Johnson syndrome. If a severe hypersensitivity reaction is suspected, discontinue this product, assess for other potential causes for the event, and initiate alternative treatment for diabetes.
The skin of tablets may come out through feces, and patients should be informed in advance that this is a normal phenomenon. The inactive portion (excipients) of this product may be excreted in the form of soft hydrates looking like the tablets through feces. If this material is found repeatedly in feces, it should be reported to the health care professional. If it was reported repeatedly by a patient that the product was found in feces, the health care professional should evaluate whether the glycemic control is being properly made.
Others: No animal studies have been conducted with the combined products in Gemigliptin/Metformin HCl to evaluate carcinogenesis, mutagenesis or impairment of fertility. The following data are based on the findings in studies with gemigliptin and metformin individually. Gemigliptin: A two-year carcinogenicity study was conducted in male and female rats given oral doses of gemigliptin of 50,150, and 450 mg/kg/day. No evidence of carcinogenicity with gemigliptin was found in either male or female rats. This dose results in exposures approximately 129~170 times the human exposure at the maximum recommended daily adult human dose (MRHD) of 50 mg/day based on AUC comparisons. A 6-month carcinogenicity study has been performed in TgrasH2 transgenic mice at doses of 200, 400, and 800 mg/kg/day in males and 200, 600, and 1200 mg/kg/day in females. There was no evidence of carcinogenicity with gemigliptin at a dose of 1200 mg/kg/day, approximately 87 times the human exposure at the maximum recommended daily dose.
Genotoxicity assessments in the Ames test, chromosomal aberrations test and in vivo micronucleus tests in mice and rats were negative.
The fertility of gemigliptin was not affected at dose of 800 mg/kg/day in rat. Gemigliptin was not teratogenic up to 200 mg/kg/day in rats and 300 mg/kg/day in rabbits, which are respectively 83 and 153 times human exposure at the MRHD of 50 mg/day.
Gemigliptin at dose of 800 mg/kg/day in rat, approximately 264 times human patient exposure at the MRHD of 50 mg/day, increased the incidence of fetus cleft palate malformation, dilated renal pelvis, misshapen thymus and sternoschisis with increasing dose.
Metformin: Long-term carcinogenicity studies have been performed in rats (dosing duration of 104 weeks) and mice (dosing duration of 91 weeks) at doses up to and including 900 mg/kg/day and 1500 mg/kg/day, respectively. These doses are both approximately four times the maximum recommended human daily dose of 2000 mg based on body surface area comparisons. No evidence of carcinogenicity with metformin was found in either male or female mice. Similarly, there was no tumorigenic potential observed with metformin in male rats. There was, however, an increased incidence of benign stromal uterine polyps in female rats treated with 900 mg/kg/day.
There was no evidence of a mutagenic potential of metformin in the following in vitro tests: Ames test (S. typhimurium), gene mutation test (mouse lymphoma cells), or chromosomal aberrations test (human lymphocytes). Results in the in vivo mouse micronucleus test were also negative.
Fertility of male or female rats was unaffected by metformin when administered at doses as high as 600 mg/kg/day, which is approximately three times the maximum recommended human daily dose based on body surface area comparisons.
Use in Children: Safety and effectiveness in children and adolescents have not been established.
Use in the Elderly: Gemigliptin/Metformin HCl: Aging can be associated with reduced renal function. Because metformin is contraindicated in patients with renal dysfunction, renal function should be carefully monitored in the elderly and should be used with caution as age increases.
Gemigliptin: Of the total number of subjects (N=1,605) in Phase II and III clinical studies of gemigliptin, 306 patients (191%) were 65 years and over. The efficacy and safety of gemigliptin were not different between young and elderly patients. However, caution should be used in elderly patient because physiological functions including liver and kidney are usually decreased in this population.
Metformin: Controlled clinical studies of metformin did not include sufficient numbers of elderly patients to determine whether they respond differently from younger patients, although other reported clinical experience has not identified differences in responses between the elderly and younger patients. Metformin is known to be substantially excreted by the kidney and because the risk of lactic acidosis to the drug is greater in patients with impaired renal function, Gemigliptin/Metformin HCl should only be used in patients with normal renal function. Because aging is associated with reduced renal function, the initial and maintenance dosing of metformin should be conservative. Care should be taken in dose selection and should be based on careful and regular monitoring of renal function.
Pregnancy: Gemigliptin/Metformin HCl: There are no adequate and well-controlled studies in pregnant women with Gemigliptin/Metformin HCl or each components of this drug. No animal studies have been conducted with the combined products in Gemigliptin/Metformin HCl to evaluate effects on reproduction. Gemigliptin/Metformin HCl should be used during pregnancy only if clearly needed.
Gemigliptin: Reproduction studies in rats and rabbits indicated that gemigliptin was transferred to placenta and up to 48.1% and 1.6% were detected in amniotic fluids when administered to pregnant rats and rabbits, respectively, at 2 hours post dose; therefore, use of gemigliptin is not recommended during pregnancy.
Metformin: Metformin was not teratogenic in rats and rabbits at doses up to 600 mg/kg/day, which represent 2 and 6 times the maximum recommended human daily dose of 2000 mg based on body surface area comparison for rats and rabbits, respectively. Determination of fetal concentrations demonstrated a partial placental barrier to metformin.
Nursing Mothers: No studies in lactating animals have been conducted with Gemigliptin/Metformin HCl. In animal studies, gemigliptin was excreted at a ratio of 1:4-10 in plasma and milk in lactating rats. Therefore, Gemigliptin/Metformin HCl should not be administered in nursing woman. It is not known whether gemigliptin or metformin are excreted in human milk.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Monotherapy and additional combination therapy: Gemigliptin: Two placebo-controlled monotherapy studies, one of 12- and one of 24-week duration, included patients treated with gemigliptin 50 mg once daily. Table 1 summarizes the most common (≥3% of patients) adverse reactions reported in the group treated with gemigliptin 50 mg once daily. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The 24-week monotherapy study was extended through 52-week. The adverse events that increased more than 1% during the latter 28 weeks when compared with the first 24 weeks, regardless of assessment of causality, were nasopharyngitis (4.44% vs 6.1%), upper respiratory tract infection (11% vs 6.1%) and increase in blood creatine phosphokinase (2.22% vs 4.88%). No new adverse events were reported in more than 2 patients (2.44%) in latter 28 weeks.
One active-controlled add-on combination therapy study with metformin included patients treated with gemigliptin 25 mg twice daily, gemigliptin 50 mg once daily and sitagliptin 100 mg once daily. Table 2 summarizes the most common (≥3% of patients) adverse reactions reported in this study. (See Table 2.)
Click on icon to see table/diagram/image
The 24-week add-on combination therapy was extended through 52-week with gemigliptin 50 mg once daily added on to stable dose of metformin. The adverse events that increased more than 1% during the latter 28 weeks when compared with the first 24 weeks, regardless of assessment of causality, were diarrhea (0.71% vs 2.7%), urinary tract infection (0.71% vs 1.8%), hypoglycemia (0.71% vs 2.7%), dizziness (0.71% vs 3.6%) and nausea (1.43% vs 2.7%). The adverse events reported in more than 2 patients (1.8%) during the latter 28 weeks were asthenia (1.8%) and myalgia (1.8%).
No clinically meaningful changes in vital signs or in ECG (including in QTc interval) were observed in patients treated with gemigliptin.
Gemigliptin 50 mg was given in patients inadequately controlled on their maximal tolerated dose of metformin and a glimepiride for 24 weeks. Table 3 summarizes the most common (≥3% of patients) adverse reactions reported in this study. (See Table 3.)
Click on icon to see table/diagram/image
In a 12-week study conducted in patients with mild and moderate renal impairment, gemigliptin 50 mg was given and Table 4 summarizes the most common (≥3% of patients) adverse reactions reported in this study. (See Table 4.)
Click on icon to see table/diagram/image
Metformin: In placebo-controlled clinical trials of extended-release metformin monotherapy, adverse reactions including diarrhea and nausea/vomiting were reported in greater than 5% of the metformin patients and that were more common in metformin than placebo treated patients (diarrhea 9.6% vs 2.6%, nausea/vomiting 6.5% vs 1.5%). Diarrhea led to discontinuation of study medication in 0.6% of patients treated with extended-release metformin.
Initial combination therapy: In a 24 weeks clinical trial that studied initial combination of metformin, gemigliptin 50 mg and metformin were individually administered and co-administered once daily. Table 5 summarizes the most common (≥3% of patients) adverse reactions reported in this study. (See Table 5.)
Click on icon to see table/diagram/image
Hypoglycemia: Gemigliptin: In two placebo-controlled clinical studies, one of 12- and one of 24-week duration, of gemigliptin 50 mg once daily as monotherapy, 2 patients (1.59%) reported hypoglycemia. One patient (0.71%) reported hypoglycemia in 24-week active-controlled add-on combination study. In the 24-week study of initial therapy, gemigliptin 50 mg once daily with metformin to a maximum dose of 2000 mg, hypoglycemia was reported in 3 patients (2.13%). In the extended 52-week studies of gemigliptin 50 mg once daily, 3 patients (2.7%) reported hypoglycemia. 10 patients (9.35%) reported hypoglycemia when gemigliptin 50 mg was given once daily as an add-on therapy in patients with inadequate glycemic control with metformin and sulfonylurea dual therapy. In a 12-week study conducted in patients with mild and moderate renal impairment, 9 patients (13.6%) reported hypoglycemia in the group treated with gemigliptin 50 mg and six patients (9.1%) in the placebo group. In the 52-week extension study where those previously receiving placebo were switched to linagliptin, 10 patients (20.0%) in the group treated with gemigliptin 50 mg reported hypoglycemia, whereas 15 patients (28.9%) reported hypoglycemia in the active comparator group. The hypoglycemia experienced by patients in clinical trials was considered mostly mild in severity and patients fully recovered.
Subjects with inadequate glycemic control on insulin monotherapy or dual therapy with insulin plus metformin were studied with add-on therapy of Gemigliptin administered once daily for 24 weeks.
The incidence rates of hypoglycaemia were 29 subjects (15.1%) in the gemigliptin group and 15 subjects (15.6%) in the placebo group. The symptomatic hypoglycaemias reported were of mild or moderate severity as the incidence rates of hypoglycaemia accompanied by symptoms (symptomatic hypoglycaemia) were 11 subjects (5.7%) in the gemigliptin group and 5 subjects (5.2%) in the placebo group. Most of the subjects recovered from these events during the study, and most of the events were deemed unrelated to the investigational drug. The incidence rates of hypoglycaemia not accompanied by symptoms (asymptomatic hypoglycaemia) were 21 subjects (10.9%) in gemigliptin group and 10 subjects (10.4%) in the placebo group.
Hypersensitivity reaction: Gemigliptin: In a 24-week active-controlled add-on combination study, two patients (1.71%) receiving 25 mg gemigliptin twice daily on a stable dose of metformin in the first 24-week and 50 mg once daily in the remaining 28 weeks reported hypersensitivity reactions, which was not related to gemigliptin exposure.
Pancreatitis: Gemigliptin: In clinical studies of sitagliptin, a member of dipeptidyl peptidase 4 (DPP-4) inhibitors, the incidence of acute pancreatitis was 0.1 per 100 patient-years (4 patients with an event in 4708 patient-years for sitagliptin treated group). In two placebo-controlled studies, one of 12-week and one of 24-week duration, of gemigliptin 50 mg once daily as monotherapy, 1 patient (1.59%) reported acute pancreatitis, which was not related to gemigliptin exposure.
Vitamin B12: Metformin: Metformin may lower Vitamin B12 levels. Measurement of hematologic parameters on an annual basis is advised in patients on Gemigliptin/Metformin HCl and any apparent abnormalities should be appropriately investigated and managed.
Bullous pemphigoid: Gemigliptin: In the post-marketing surveillance in the patients treated with other DPP-4 inhibitors, bullous pemphigoid requiring hospitalization has been reported.
Results of post-marketing surveillance in Korea (gemigliptin tartrate (single agent, for oral administration)): In the results of post-marketing surveillance conducted in 3,036 subjects for 6 years as the re-examination of gemigliptin tartrate (single agent, for oral administration) in Korea, the incidence of adverse events was reported to be 8.17% (248/3,036 subjects, 328 cases in total) regardless of causality. Among them, the serious adverse events regardless of causality are listed in table 6. No serious adverse drug reactions for which the causality could not be excluded were reported. (See Table 6.)
Click on icon to see table/diagram/image
In addition, the unexpected adverse events regardless of causality and the unexpected adverse drug reactions for which the causality could not be excluded are listed in the table as follows. (See Table 7.)
Click on icon to see table/diagram/image
Results of post-marketing surveillance in Korea (gemigliptin tartrate and metformin hydrochloride (combination agents, for oral administration): In the results of post-marketing surveillance conducted in 624 subjects as the re-examination of gemigliptin tartrate and metformin hydrochloride (combination agents, for oral administration) in Korea, the incidence of adverse events was reported to be 5.45% (34/624 subjects, 43 cases in total) regardless of causality. Among them, neither serious adverse events regardless of causality nor serious adverse drug reactions for which the causality could not be excluded were reported.
In addition, the unexpected adverse events regardless of causality and the unexpected adverse drug reactions for which the causality could not be excluded are listed in the table 8. (See Table 8.)
Click on icon to see table/diagram/image
Domestic and foreign post-marketing spontaneous reports: The followings are the adverse events which were additionally identified during postmarketing use of the product. Because these events are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure: Pruritus, Rash and Urticaria.
Co-administration of single dose of gemigliptin (50 mg) and metformin (1 g) given twice daily did not meaningfully alter the pharmacokinetics of either gemigliptin or metformin in healthy volunteers.
Pharmacokinetic drug interaction studies with Gemigliptin/Metformin HCl have not been performed; however, such studies have been conducted with the individual components.
Gemigliptin: The responsible enzyme for the metabolism of gemigliptin is CYP3A4. In vitro studies indicated that gemigliptin is not an inhibitor of CYP1A2, 2A6, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A4 and is not an inducer of CYP1A2, 2C8, 2C9, 2C19, or 3A4. Therefore, gemigliptin is unlikely to cause interactions with other drugs that utilize these metabolic pathways. In vitro studies further indicated that gemigliptin did not induce p-glycoprotein (p-gp) while mildly inhibited p-gp mediated transport at high concentration. Therefore, gemigliptin is unlikely to cause interactions with other P-gp substrates at therapeutic concentrations.
Effects of gemigliptin on other drugs: In clinical studies, gemigliptin did not meaningfully alter the pharmacokinetics of metformin, pioglitazone, glimepiride, rosuvastatin, dapagliflozin, and empagliflozin providing in vivo evidence of a low propensity for causing drug interactions with substrates of CYP2C8, CYP2C9, CYP3A4, and organic cation transporter (OCT).
Metformin: Co-administration of multiple doses of 50 mg gemigliptin with 2000 mg metformin, a substrate of OCT1 and OCT2, to steady state decreased the Cmax of metformin by 13% but did not affect the AUC of metformin.
Pioglitazone: Co-administration of multiple doses of 200 mg gemigliptin with 30 mg pioglitazone, a substrate of CYP2C8 and 3A4, to steady state decreased the AUC and Cmax of pioglitazone by 15% and 17%, respectively. However, those of the active metabolites of pioglitazone were not changed.
Glimepiride: Co-administration of multiple doses of 50 mg gemigliptin to steady state with a single dose of 4 mg glimepiride, a substrate of CYP2C9, did not meaningfully alter the pharmacokinetics of glimepiride.
Rosuvastatin: Co-administration of multiple doses of 50 mg gemigliptin with 20 mg rosuvastatin, a substrate of CYP2C9 and 3A4, to steady state did not meaningfully alter the pharmacokinetics of rosuvastatin.
Repeated co-administration of 50 mg gemigliptin with 10 mg of dapagliflozin, substrate of UGT149, did not meaningfully alter the pharmacokinetics of dapagliflozin at steady state.
Repeated co-administration of 50 mg gemigliptin with 25 mg of empagliflozin, substrate of UGT2B7, UGT1A3, UGT1A8, and UGT1A9, did not meaningfully alter the pharmacokinetics of empagliflozin at steady state.
Effects of other drugs on gemigliptin: In clinical studies, metformin, pioglitazone, rosuvastatin, dapagliflozin, and empagliflozin did not meaningfully alter the pharmacokinetics of gemigliptin. Ketoconazole did not meaningfully alter the pharmacokinetics of gemigliptin. Therefore, strong and moderate CYP3A4 inhibitors would not cause clinically meaningful drug interactions. Rifampicin (rifampin), on the other hand, significantly decreased exposure of gemigliptin. Therefore, co-administration with other strong CYP3A4 inducers, including rifampicin (rifampin), dexamethasone, phenytoin, carbamazepine, rifabutin and phenobarbital, is not recommended.
Metformin: Co-administration of 50 mg gemigliptin with 2000 mg metformin, a substrate of OCT1 and OCT2, to steady state did not meaningfully alter the pharmacokinetics of gemigliptin.
Pioglitazone: Co-administration of 200 mg gemigliptin with 30 mg of pioglitazone, a substrate of CYP2C8 and 3A4, to steady state did not meaningfully alter the pharmacokinetics of gemigliptin.
Ketoconazole: Co-administration of multiple doses of 400 mg ketoconazole once daily, a strong inhibitor of CYP3A4, to steady state with a single dose of 50 mg gemigliptin, increased the AUC of active moiety, the sum of gemigliptin and its active metabolite by 19-fold.
Rifampicin: Co-administration of multiple doses of 600 mg rifampicin once daily, a strong inducer of CYP3A4, to steady state, with a single dose of 50 mg gemigliptin, decreased the AUC and Cmax of gemigliptin by 80% and 59%, respectively. The Cmax of active metabolite of gemigliptin was not significantly affected while the AUC was decreased by 41%.
Rosuvastatin: Repeated administration of 20 mg of rosuvastatin, a strong inducer of CYP2C9 and 3A4, with 50 mg of gemigliptin to steady state did not meaningfully alter the pharmacokinetics of gemigliptin.
Repeated co-administration of 50 mg gemigliptin with 10 mg of dapagliflozin, substrate of UGT1A9, did not meaningfully alter the pharmacokinetics of dapagliflozin at steady state.
Repeated co-administration of 50 mg gemigliptin with 25 mg of empagliflozin, substrate of UGT2B7, UGT1A3, UGT1A8, and UGT1A9, did not meaningfully alter the pharmacokinetics of empagliflozin at steady state.
Metformin: Concomitant medication(s) of below medicinal products may potential hypoglycemic or hyperglycemic effects of metformin. Therefore, co-administration should be based on a careful assessment of glucose level and patient monitoring.
Drugs that can potentiate the hypoglycemic effect of metformin: Insulin, sulfonylamides, sulfonylureas, alpha-glucosidase inhibitors, anabolic steroid, guanethidine, salicylates (aspirin) beta blockers (propranolol), MAO inhibitors, angiotensin receptor antagonists.
Drugs that can potentiate the hyperglycemic effect of metformin: Epinephrine, sympathomimetics, corticosteroids, thyroid hormones, follicle hormone, estrogen, oral contraceptives, thiazides and other diuretics, pyrazinamide, isoniazid, nicotinic acid, phenothiazines, phenytoin, calcium channel blocking drugs.
Alcohol: The risk of metformin accumulation and lactic acidosis increases in patients with acute alcohol intoxication in the following conditions: Fasted or malnourished state; Reduced hepatic function.
Intake of alcohol or medicinal products that contain alcohol should be avoided.
Iodinated contrast agents: The intravascular administration of iodinated contrast agents in radiological studies may lead to renal failure, resulting in metformin accumulation and a risk of lactic acidosis. Therefore, Gemigliptin/Metformin HCl must be discontinued prior to, or at the time of the test and not reinstituted until 48 hours afterwards, and only after renal function has been re-evaluated and found to be normal.
Glyburide: In a single-dose interaction study in type 2 diabetes patients, coadministration of metformin and glyburide did not result in any changes in either metformin pharmacokinetics or pharmacodynamics. Decreases in glyburide AUC and Cmax were observed, but were highly variable. The single-dose nature of this study and the lack of correlation between metformin blood levels and pharmacodynamics effects, makes the clinical significance of this interaction uncertain.
Furosemide: A single-dose, metformin-furosemide drug interaction study in healthy subjects demonstrated that pharmacokinetic parameters of both compounds were affected by coadministration. Furosemide increased the metformin plasma and blood Cmax by 22% and blood AUC by 15%, without any significant change in metformin renal clearance. When administered with metformin, the Cmax and AUC of furosemide were 31% and 12% smaller, respectively, than when administered alone, and the terminal half-life was decreased by 32%, without any significant change in furosemide renal clearance. No information is available about the interaction of metformin and furosemide when coadministered chronically.
Nifedipine: A single-dose, metformin-nifedipine drug interaction study in normal healthy volunteers demonstrated that coadministration of nifedipine increased plasma metformin Cmax and AUC by 20% and 9%, respectively, and increased the amount excreted in the urine. Tmax and half-life were unaffected. Nifedipine appears to enhance the absorption of metformin. Metformin had minimal effects on Nifedipine.
Drugs which may affect renal function, cause significant hemodynamic changes, or affect metformin such as organic cation transporter excreted through renal tubular secretion: Metformin is a substrate of organic cation transporter (OCT) 1 and OCT 2.
Concomitant use with OCT1 inhibitors (verapamil, etc.) may reduce the effect of metformin.
Concomitant use with OCT1 inducers (rifampicin, etc.) may increase the gastrointestinal uptake and effect of metformin.
Concomitant use with OCT2 inhibitors (cimetidine, dolutegravir, lanolazine, trimethoprim, vandetanib, isavuconazole, etc.) may reduce the renal excretion of metformin leading to increase in blood concentration of metformin.
Concomitant use with OCT2 & OCT1 co-inhibitors (crizotinib, olaparib, etc.) may affect the renal excretion and effect of metformin.
Therefore, as concomitant use with such medicines may increase the blood concentration of metformin, special caution is required, especially for patients with renal impairment. As OCT inhibitors/inducers may change the effect of metformin, dose adjustment of metformin may be considered if necessary.
In addition, non-steroidal anti-inflammatory drugs (NSAIDs), angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists, diuretics (especially loop diuretics), etc. may have adverse effects on renal function leading to increase in the risk of lactic acidosis, renal function should be closely monitored when they are administered concomitantly with metformin.
Others: In healthy volunteers, the pharmacokinetics of metformin and propranolol, and metformin and ibuprofen were not affected when coadministered in single-dose interaction studies. Metformin is negligibly bound to plasma proteins and is, therefore, less likely to interact with highly protein-bound drugs such as salicylates, sulfonamides, chloramphenicol, and probenecid, as compared to the sulfonylureas, which are extensively bound to serum proteins.
Precautions about storage and carrying: Store in the originally purchased container. Placing in container other than the ones provided by the manufacturer may lead to drug misuse or affect the quality of the drug product.
Store at room temperature (30°C) in tight container.
Shelf-Life: Effective for 36 months from the date of manufacture.
A10BD18 - metformin and gemigliptin ; Belongs to the class of combinations of oral blood glucose lowering drugs. Used in the treatment of diabetes.
Zemimet SR FC tab
28's (P49.95/film-coated tab)




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image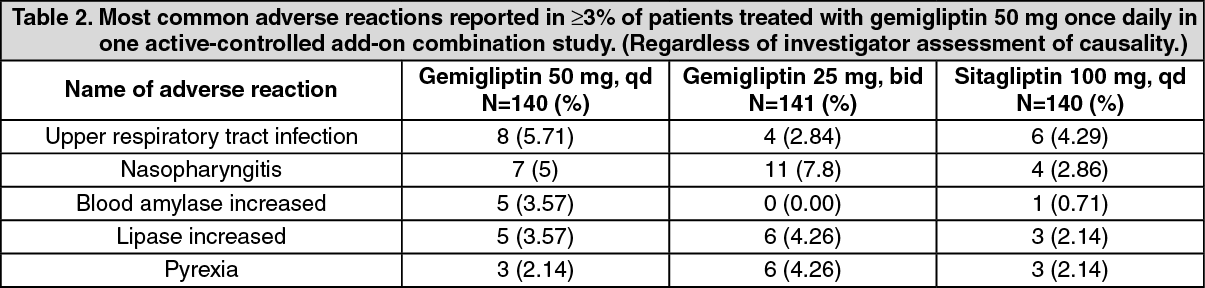 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image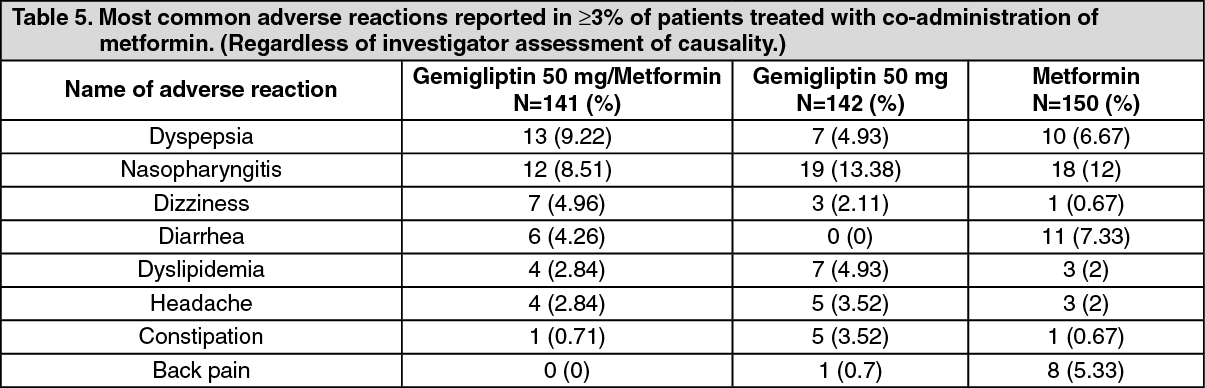 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image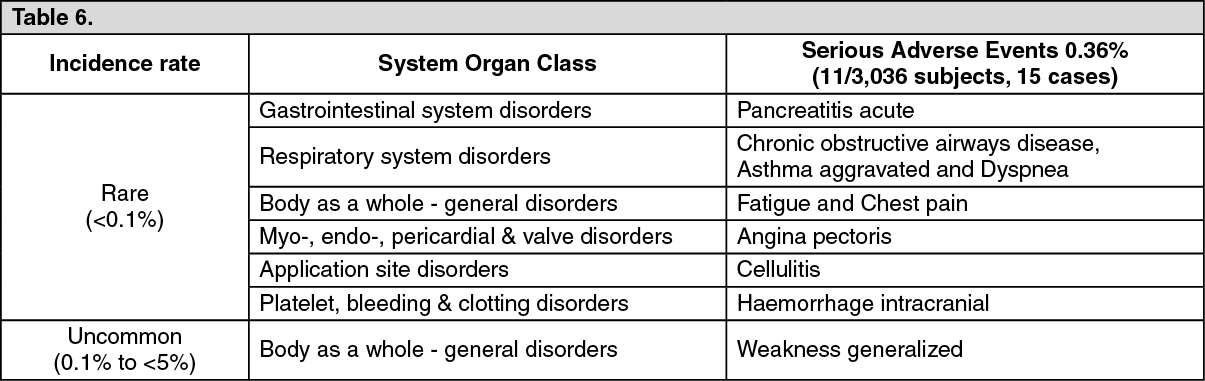 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image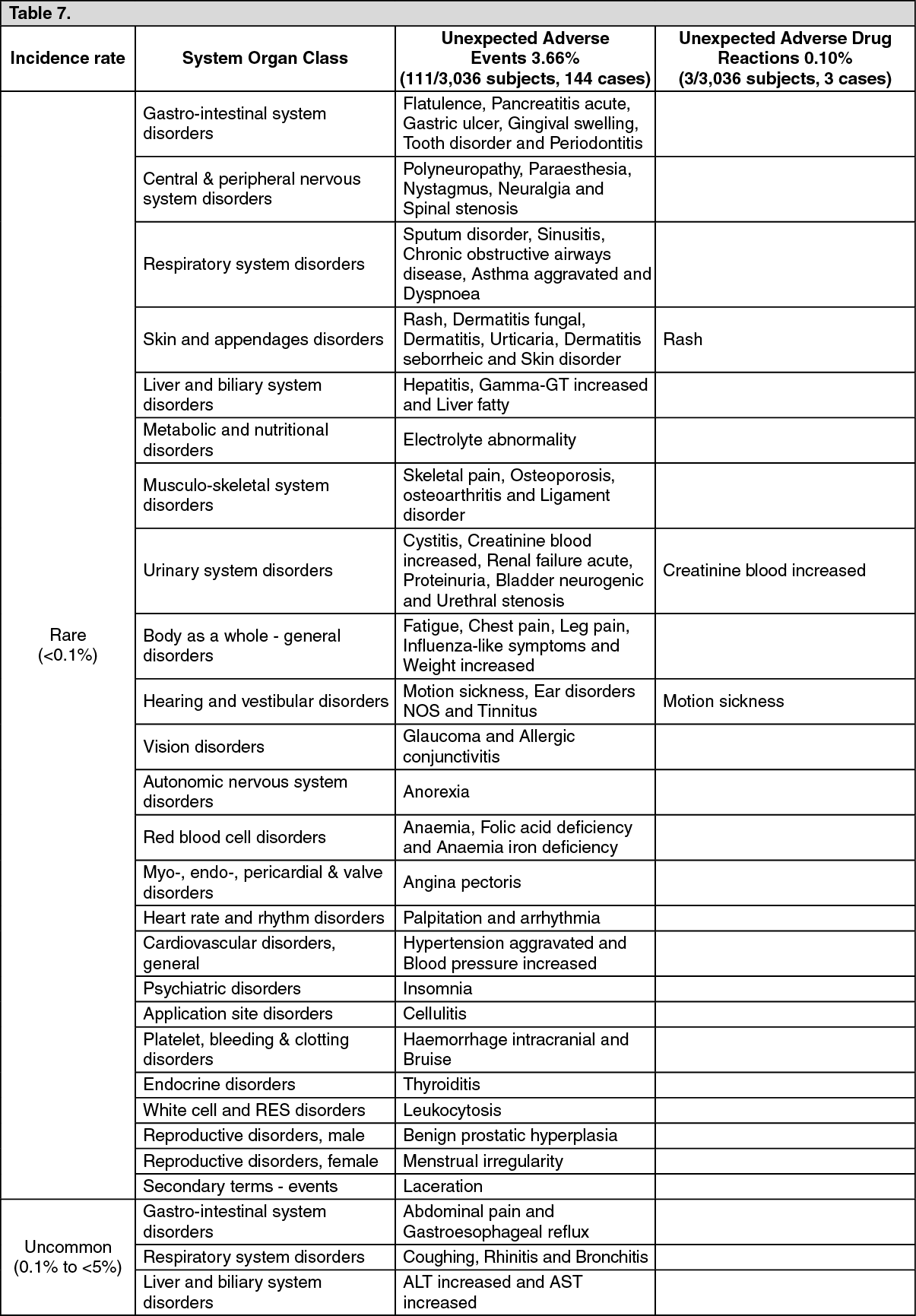 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image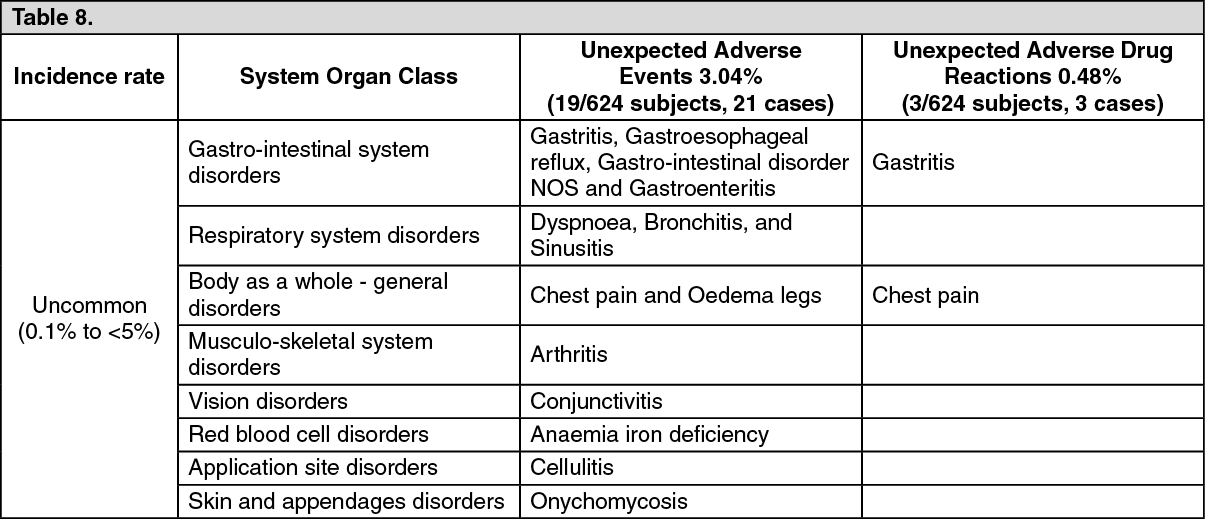 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
